
こんにちは!
運動器専門のリハビリスタッフです!!
いつもお世話になります。
今回は、『ランナー膝(腸脛靭帯炎)は本当に大腿筋膜張筋の筋活動が高いのか?』
について解説させていただきます。
ランナー膝(腸脛靭帯炎)は主に膝の外側が痛くなる症状であり、腸脛靭帯に対するオーバーユース(過用)であるとされています。
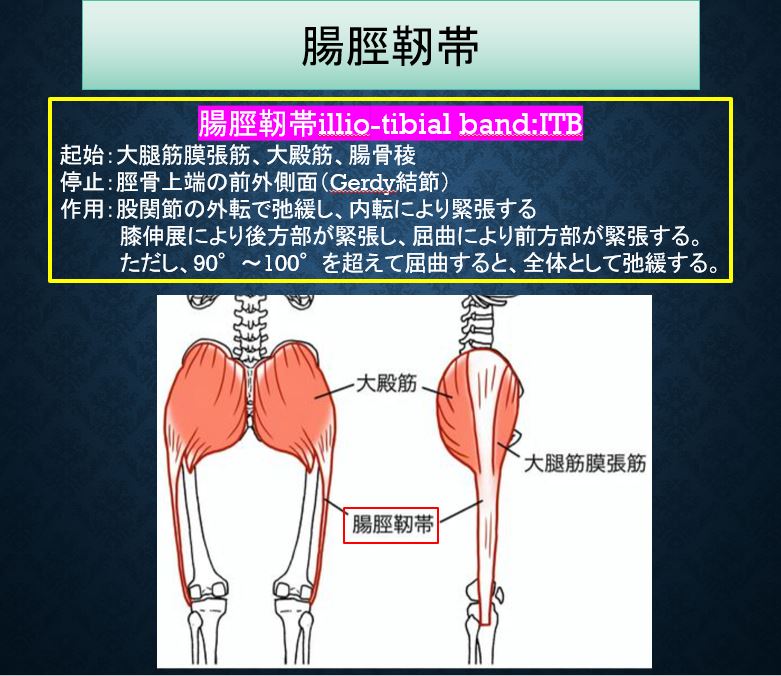
腸脛靭帯Iliotibial band (ITB)は大腿外側組織である大殿筋、中殿筋、大腿筋膜張筋、外側広筋の筋膜が合流して、分厚くなった組織です。
腸脛靭帯は大殿筋、大腿筋膜張筋から起始し、膝に近い脛骨前外側部の隆起であるGerdy結節に停止します。
ランナー膝(腸脛靭帯炎)は主にランニングによる膝関節周辺傷害のひとつです。
膝関節の屈伸を繰り返すことで、腸脛靭帯が大腿骨外顆と接触することで滑膜炎(炎症)を起こし、疼痛が発生するとされています。
特に膝関節屈曲30°付近で腸脛靭帯後縁と大腿骨外側上顆との摩擦が強く、痛みが生じやすくなっております。
海外では腸脛靭帯症候群Iliotibial band syndrome (ITBS)と表現されることが多いようです。
マラソンやバスケットボール、自転車競技等のアスリートに発生しやすいとされています。
大腿骨外顆での圧痛やgrasping test(大腿骨外顆部で腸脛靭帯を圧迫し膝を90°屈曲位から伸展させる)、Ober testで疼痛が誘発されることが多いです。
『Oberテスト変法の方法と有用性』https://undoukirehazemi.com/%e3%80%8eobel%e3%83%86%e3%82%b9%e3%83%88%e5%a4%89%e6%b3%95%e3%81%ae%e6%96%b9%e6%b3%95%e3%81%a8%e6%9c%89%e7%94%a8%e6%80%a7%e3%80%8f/
外因性の要因として走行距離や頻度の急激な増加、踵の外側が摩耗した靴の使用などが報告されています
内因性の要因として内反膝、回外足、大腿筋膜張筋の短縮や中殿筋筋力不足などが報告されています。
そんな中、2018年に、ランナー膝(腸脛靭帯炎)症例に対して、ランニング中の筋活動を筋電図にて解析し、検証した論文が海外で報告されております。
この論文の検証結果が気になるところです。
◆論文紹介
Observational Study
PM R (IF: 2.3; Q3)
. 2018 Oct;10(10):1032-1039.
doi: 10.1016/j.pmrj.2018.04.004. Epub 2018 Apr 26.
Differences in Knee and Hip Adduction and Hip Muscle Activation in Runners With and Without Iliotibial Band Syndrome
腸脛靱帯症候群の有無によるランナーの膝・股関節の内転と股関節筋の活性化の違い
Robert L Baker 1, Richard B Souza 2, Mitchell J Rauh 3, Michael Fredericson 4, Michael D Rosenthal 3
Affiliations expand
- PMID: 29705166 DOI: 10.1016/j.pmrj.2018.04.004
Abstract
Background: Iliotibial band syndrome has been associated with altered hip and knee kinematics in runners. Previous studies have recommended further research on neuromuscular factors at the hip. The frontal plane hip muscles have been a strong focus in strength comparison but not for electromyography investigation.
概要
背景 腸脛靱帯症候群は、ランナーにおける股関節および膝関節の運動学的変化と関連しています。これまでの研究では、股関節の神経筋の要因についてさらなる研究が推奨されています。前額面の股関節筋は筋力比較では強く注目されているが、筋電図調査では注目されていない。
Objective: To compare hip surface electromyography, and frontal plane hip and knee kinematics, in runners with and without iliotibial band syndrome.
目的 腸脛靱帯症候群の有無にかかわらず、ランナーにおける股関節表面筋電図、および股関節と膝関節の前額面運動特性を比較すること。
Design: Observational cross-sectional study.
デザイン 観察的横断研究。
Setting: Biomechanics research laboratory within a university.
設定 大学内のバイオメカニクス研究室。
Participants: Thirty subjects were recruited consisting of 15 injured runners with iliotibial band syndrome and 15 gender-, age-, and body mass index-matched controls. In each group, 8 were male runners and 7 were female runners. Inclusion criteria for the injured group were pain within 2 months related to iliotibial band syndrome and a positive Noble compression test. Participants were excluded if they reported other lower extremity diagnoses within the last year or active lower extremity or low back pain not related to iliotibial band syndrome. Controls were excluded if they reported a history of iliotibial band syndrome. Convenience sampling was used based on referrals from local running clinics and orthopedic clinics.
参加者。腸脛靱帯症候群を発症したランナー15名と、性別、年齢、肥満度をマッチさせた対照者15名、計30名が対象となった。各群とも、男性ランナー8名、女性ランナー7名であった。傷害群の参加基準は、腸脛靱帯症候群に関連する2ヶ月以内の痛みとNoble compression testが陽性であることであった。参加者は、過去1年以内に他の下肢の診断を受けていた場合、または腸脛靱帯症候群に関連しない下肢または腰痛の活動性を報告した場合は除外された。対照者は、腸脛靱帯症候群の既往を報告している場合は除外した。地元のランニングクリニックや整形外科クリニックからの紹介によるコンビニエンスサンプリングが行われた。
Methods: Three-dimensional motion capture was performed with 10 high-speed cameras synchronized with wireless surface electromyography during a 30-minute run. The first data point was at 3 minutes, using a constant speed of 2.74 meters per second. A second data point was at 30 minutes, using a self-selected pace by the participant to allow for a challenging run until completion at 30 minutes.
方法 30分のランニング中に、ワイヤレス表面筋電図と同期した10台の高速カメラで3次元モーションキャプチャーを行った。最初のデータポイントは3分で、毎秒2.74mの一定速度を使用した。2回目のデータポイントは30分で、参加者が自分で選択したペースを使用し、30分で完了するまで挑戦的なランニングができるようにした。
Main outcome measurements: Motion capture was reported as peak kinematic values from heel strike to peak knee flexion for hip adduction and knee adduction. Surface electromyography was reported as a percentage of maximal voluntary contraction for the gluteus maximus, gluteus medius and tensor fascia latae muscles.
主なアウトカム測定 モーションキャプチャは、股関節内転および膝関節内転の踵接地から膝関節屈曲までの運動量のピーク値として報告された。表面筋電図は、大殿筋、中殿筋、大腿筋膜張筋の最大自発収縮率として報告された。
Results: Injured runners demonstrated increased knee adduction compared with control runners at 30 minutes (P = .002, control = -1.48°, injured = 3.74°). Tensor fasciae latae muscle activation in injured runners was increased compared with control runners at 3 minutes (P = .017, control = 7% maximal voluntary isometric contraction, injured = 11% maximal voluntary isometric contraction).
結果 負傷したランナーは、30分後に対照ランナーに比べて膝関節の内転が増加した(P = .002、対照=-1.48°、負傷=3.74°)。負傷したランナーの大腿筋膜張筋の活性化は、3分後に対照ランナーと比較して増加した(P = .017、対照=7%の最大随意筋収縮、負傷=11%の最大随意筋収縮)。
◆論文の結論
Conclusion: The results of this study suggest that lateral knee pain in runners localized to the distal iliotibial band is associated with increased knee adduction at 30 minutes. Increased tensor fasciae latae muscle activation at 3 minutes is noted, but more investigation is needed to better understand the clinical meaning. These findings are consistent with but not conclusive evidence supporting the theory that neuromuscular factors of the hip muscles may contribute to increased knee adduction in runners with iliotibial band syndrome. We advise caution using these findings to support treatments intended to modify tensor fasciae latae activation, given the small differences of 4% in muscle activation. Increased knee adduction in runners at 30 minutes was over 5° and beyond the minimal detectable difference. Additional research is needed to confirm whether the degree of knee adduction changes earlier versus later in a run and whether fatigue is a clinically relevant factor.
結論 本研究の結果は、ランナーにおける遠位腸脛靱帯に限局した膝外側の疼痛は、30分後の膝関節内転の増加と関連していることを示唆している。3分後の大腿筋膜張筋の活性化が認められるが、臨床的な意味をより深く理解するためには、さらなる調査が必要である。これらの知見は、腸脛靱帯症候群のランナーにおいて、股関節の筋肉の神経筋的要因が膝関節内転の増加に寄与しているという説を支持する決定的な証拠とはならないが、一致するものである。また、大腿筋膜張筋の活性化を修正することを目的とした治療をサポートするために、これらの知見を用いることは、筋の活性化における4%というわずかな差を考慮すると、注意が必要である。30分後のランナーにおける膝関節内転の増加は、5°以上であり、最小検出可能差を超えるものであった。ランニングの初期と後期で膝関節内転の程度が変化するかどうか、また、疲労が臨床的に関連する要因であるかどうかを確認するためには、さらなる研究が必要である。
◆まとめ
上記論文ではランナー膝15名(男性8名、女性7名)と対照者15名(男性8名、女性7名)の計30名に対して、30分のランニング中に表面筋電図(大殿筋、中殿筋、大腿筋膜張筋)および3次元モーションキャプチャーにて股関節内転および膝関節内転(内反)の踵接地から膝関節屈曲までの運動量のピーク値を測定しております。
結果としてランニング30分後、ランナー膝症例は対照者と比較すると、膝関節の内転(内反)が5°以上有意に増加しており、ランニング3分後には大腿筋膜張筋の筋活動は増加していたとのことです。
上記論文の結果を踏まえると、ランナー膝症例はランニング中に大腿筋膜張筋の筋活動が高く、膝関節が内反になる傾向があることがわかりました。
上記の研究結果は、ある程度予想通りの結果にはなっていますね。
やはり、ランナー膝へは運動療法やインソール等で大腿筋膜張筋への負荷量を減らすなどの対応策が必要かもしれませんね。
今回は、『ランナー膝(腸脛靭帯炎)は本当に大腿筋膜張筋の筋活動が高いのか?』
について解説させていただきました。

